- Informace k fixaci pomocí Opencastu
Máte-li zájem o fixaci zlomeniny u dítěte pomocí Opencastu, kontaktujte nás prosím e-mailem. K posouzení vhodnosti této metody a k domluvě termínu potřebujeme následující informace:
- věk dítěte,
- váhu dítěte,
- typ zlomeniny,
- RTG snímky zaslané do systému Jivex Nemocnice Jihlava.
Na základě těchto údajů bude posouzena vhodnost použití Opencastu a domluven další postup.
Kontaktní e-maily:
Telefonické konzultace:
V případě potřeby nás můžete kontaktovat také telefonicky na čísle 567 157 709, a to v pondělí, středu a čtvrtek mezi 7:00 a 7:30 hodinou.
- ACP - blood plasma therapy
Autologous Conditioned Plasma - APC plasma method.
Since 2012, a method of treating joint damage with the patient's own blood plasma has been introduced. This treatment is popular in the world mainly because the active substances (the so-called growth factors that help healing) are provided by the body itself, so you are not burdened with the application of foreign chemicals, there is no risk of allergic reactions, etc.Where does it help ?
- Painful arthrosis of joints - mainly 1st and 2nd degree.
- In the healing of joint injuries - injuries to articular cartilage.
- For tendon and muscle injuries.
- Helps with symptoms of joint congestion - accelerates joint regeneration.
If you are interested, please contact our orthopaedic clinic. We will explain your options and assess whether this treatment is suitable for you.
The procedure is not covered by health insurance.
The price of 1 application is 2900 CZK, usually 3 injections are administered. - Visionaire
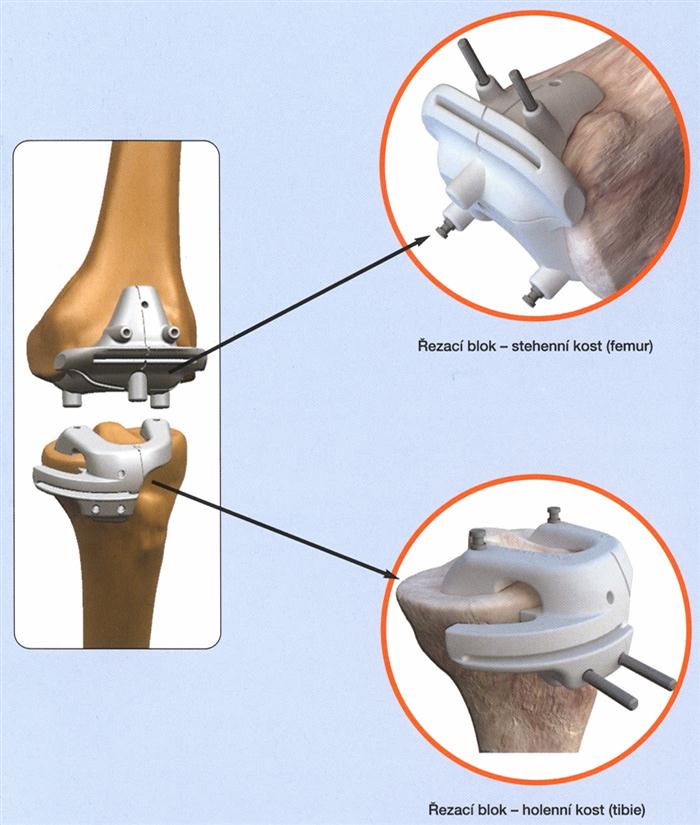
Visionaire's unique technology allows Smith & Nephew to design and manufacture a set of original cutting blocks based on the patient's own anatomy. Using a magnetic resonance imaging (MRI) scan of the patient's knee, along with a complete X-ray of the lower extremity, two cutting blocks (for the femur and tibia) are designed and fabricated to replace (arthroplasty) the patient's knee joint. This custom fitting allows the orthopaedic surgeon to make absolutely precise bone cuts in the ideal rotation and inclination required for optimal placement of the knee implant. Smith&Nephew is the first company in the Czech Republic to offer this technology, which has the necessary approval (CE certificate). The cutting blocks are made of a highly safe material - medical grade nylon and are supplied in sterile packaging along with the patient's name and number so that no confusion can occur. Currently, approximately 20,000 endoprostheses are implanted worldwide using Visionaire technology and this number is growing every day.
What are the benefits for the patient?
- Absolutely precise positioning of the implant - knee replacement, which is crucial for its proper function and durability.
- Significantly faster surgeries - reducing the time spent in the surgery room.
- Greater safety for the patient - up to 22 fewer surgical steps.
- The patient has lower blood loss (the need for blood transfusion is reduced).
- Significantly lower risk of infection due to shorter surgery time and fewer surgical instruments required.
- Shorter and more gentle anaesthesia - the patient is under its influence for a shorter period of time.
- Lower risk of other complications - fat embolism, deep vein thrombosis.
- Less invasive surgical technique (more gentle intervention into the patient's tissues and bones).
- Less painful surgery.
- Faster and more effective recovery and return to the active life.
- Orthopaedic surgery
Waiting times:
Endoprostheses of large joints (hip, knee, shoulder) 13-14 měsíců.
Arthroscopy and "minor" surgical procedures (anterior cruciate ligament replacements, corrective surgery on the hands and feet, including hallux valgus) 2-4 weeks depending on the number of patients.
Note: Minor surgery - surgery that is less invasive for the patient and usually requires a shorter hospital stay, 1-4 days.Arthroscopic surgery
These are medical and diagnostic joint surgeries performed using an arthroscope. The image is transmitted to the screen using light cables. The surgery itself is carried out with special instruments, when the joint is filled with saline by a pump.
The most frequently operated joint is the knee, followed by the shoulder, less frequently the kneecap and elbow. These surgeries are very gentle, allow quick rehabilitation and recovery, and require a very short hospital stay. The cosmetic effect is also significant - only two small wounds on the front of the knee joint.
Operations are performed in a modern surgery room equipped with an arthroscopic tower. We have special arthroscopic devices such as shaver (miniature milling machine) and Vulcan (high frequency coagulation).Arthroscopic surgery on the knee joint
Meniscus treatment
The most common arthroscopic procedure - a relatively uncomplicated surgery where the damaged part of the meniscus is either removed (partial menisectomy) or the torn meniscus is sewn back together with absorbable sutures.
The patient is discharged home the next day. After the menisectomy, the limb can be loaded according to the tolerance and immediate rehabilitation is started. In case of meniscus suture, the postoperative regime is slow due to the possibility of meniscus retear, 4-6 weeks of rigid brace, then careful rehabilitation, weight bearing, i.e. walking on the operated limb is possible immediately. In the long term it is better to preserve the meniscus. Anesthesia is spinal or general. Complications are rare.Anterior cruciate ligament surgery
Anterior cruciate ligament tears are among the most common sports injuries. The ligament is most commonly torn during rotational and uncoordinated movement. It is accompanied by pain, often a cracking feeling in the joint, limitation of mobility and early onset of swelling of the joint.
Early treatment consists first of rest, puncture of the hemarthrosis (blood in the joint), icing, bracing. If there is any diagnostic uncertainty or suspicion of concomitant meniscus damage, early arthroscopy is indicated. Suturing of the ligament showed poor results, so this method was abandoned. 4 weeks or more after the injury, ligament resurfacing, i.e. ligament reconstruction with a graft, can be performed. This is taken either from the patellar ligament (ligament under the patella) or from the hamstring (tendon on the inside of the knee), depending on the level of future sporting activity, occupation and gender. A graft can also be ordered from a tissue bank. We use a number of special and mostly absorbable implants to anchor the graft.
After surgery, immediate rehabilitation with RHB is initiated, walking and stepping according to pain tolerance, the orthotics is indicated only in some cases. Hospitalization lasts 3-4 days. Rehabilitation and strain is gradual and long term. Full sports activity is possible in 5-6 months.
Non-operative treatment consists of strengthening the thigh muscles (mainly the posterior muscle group), electrostimulation and physical therapy. A special orthotics is used for sports.Treatment of damaged cartilage
Damaged cartilage is one of the most common arthroscopic findings. In indicated cases, we cover the defect by cartilage transfer with a so-called mosaic reconstruction. Other times, a so-called cartilage debridement is performed, i.e. removal (alignment) of the damaged cartilage. For larger defects, chondrocyte from a tissue bank can be grown.
Other arthroscopic knee procedures
Removal of loose objects (joint mice), treatment of symptomatic plicas, assessment of arthritic knee involvement with regard to further surgery, treatment of intra-articular fractures, removal of swollen joint lining and its collection for histological examination.
Arthroscopic surgery on the shoulder
The method is similar to the knee joint. Usually the surgery is performed under general anaesthesia. A special traction device is used to make the joint clear. The most common procedures are the stabilization for recurrent luxations, treatment of cartilage, removal of swollen joint lining, treatment for the so-called impingement syndrome by acromioplasty, suturing of torn tendons of the rotator cuff.
Arthroscopic shoulder stabilization
In repeated dislocations of the shoulder, the joint capsule and ligaments that hold the head in the socket must be reconstructed. Previously, these surgeries were performed open, but today they are almost always performed arthroscopically. We use a variety of absorbable and titanium implants to suture or resurface the damaged structures. After surgery, the limb is fixed with a orthotics for 4-6 weeks. The patient is discharged home the day after surgery.
Acromyoplasty
As a result of joint degeneration or traumatic damage to the tendons and ligaments of the shoulder, the space between the knob and the humerus is narrowed. When lifting the arm, the knob is then impacted (impingement) into the upper arm, which is accompanied by pain. When the conservative treatment is no longer possible, a surgical solution consisting in the removal of the lower part of the humerus is indicated. Today, these surgeries are performed more arthroscopically using a special bone cutter. After this operation, immediate rehabilitation is started, but it must be taken into account that the rehabilitation of the shoulder is always longer term.
Rotator cuff sutures
Tendon damage in the brachial plexus area of the upper limb is one of the common causes of shoulder pain. Mostly the tendon of the supraspinatus muscle, which is part of the so-called rotator cuff, is torn. In indicated cases, suturing is necessary. The operation can be performed openly and, more recently, arthroscopically using special instruments. After this surgery, fixation with a orthotics for 3-6 weeks is necessary, followed by rehabilitation, which is usually longer.
- Children's hip examination
Dear Parents,
on the basis of the Methodological Instruction of the Ministry of Health of the Czech Republic from 1996, hip joints of newborns and infants are examined to exclude congenital dislocation of the hip joints. This is a serious developmental defect of the hip joint that occurs in about 5% of children. If this defect is not recognized and treated early, it leads to severe damage to the hip joint. The hip examination is carried out in 3 stages in a so-called "triple sieve system" and is performed by an orthopaedic surgeon. The examination consists of an examination of the newborn or infant and an ultrasound examination of the hip joints. The examination does not put any strain on your child and cannot cause any harm. The first stage of the examination takes place in the delivery room or after you are discharged, no later than 3 weeks of age. The second stage then follows at 6 - 9 weeks and the third stage at 12 - 16 weeks of age.If the finding on the child's hip is normal, we recommend normal wrapping. Disposable panties or the use of a regular cloth diaper are appropriate. If the examination reveals delayed hip development, this is not yet a defect that needs to be treated. In this case, we recommend a so-called wide or abduction pack. This consists of putting on 3 diapers. These then keep the child's hip in a position that guarantees the correct development.
Only when a developmental defect of the hip joints is found, we attach a therapeutic aid, which is most often the so-called abduction Frejka's blanket, or in more severe cases Pavlík's shackles. The staff of the neonatal unit will instruct you on the correct wrapping, and the orthopaedic surgeon will always instruct you on the application of the treatment aid.
If the child is treated with any of the abduction aids, attach the normal nappy. If the child is restless and cries in the first few days of treatment, remove the appliance and see the orthopaedic surgeon for an examination.
As soon as normal development of the hip joints occurs during treatment, the treatment aid is postponed. Treated children are then monitored, followed by check-ups at 3, 6 and 10 years, when an X-ray checks for normal hip joint development.
In children who have not been treated, X-rays of the hip joints are no longer performed.WEDNESDAY: 13:00 - 13:30 (For treated and untreated children)
For treated children, check-ups at 3, 6 and 10 years are carried out in the orthopaedic outpatient clinic for children at the orthopaedic department of the hospital.
- List of items needed for hospitalisation
- Health-insurance card.
- ID card.
- Sick leave, if issued.
- Toiletries.
- Crutches and other prosthetic aids (shoulder sling, etc.).
- Footwear for changing - if the use of crutches is expected, then closed shoes ( and a shoehorn) are recommended.
- Toilet paper,
- Pyjamas, nightgown.
- Personal medication.
- Elastic bandages.
Please come to the Contact Center for the admission or at weekends at the department in Block G, 3rd floor.
From your own belongings, you can use towels, radios or a tape recorder with headphones, of course books, magazines. Bring a coffee spoon, mug and cutlery if possible.
We also ask you not to bring jewellery and large amounts of money to the hospital.
If you receive an age or disability pension, arrange for your delivery post office to deposit this pension until you are released.
Women admitted for surgery, remove nail polish.Further information can be found on the hospital's website HERE.
- Rehabilitation after orthopaedic surgery
Exercise and lifestyle after total hip replacement
Dear friends,
You have just returned home from the hospital with a sense of relief that you and the team of doctors have successfully managed a rather serious operation on a painful hip joint. You are aware that your affected joint has been replaced either partially or (more commonly) completely with an artificial joint, called a total hip replacement.The aim of the surgical team was not only to relieve you of the pain in the affected joint, which had bothered you for many years and made your personal and social life uncomfortable, but also to preserve or restore the movement in the operated joint so that it is as equivalent as possible to the mobility of a healthy joint.
But how do you treat this part of your body to make it last as long as possible? First of all, you need to remember that the actual surgery was only an essential part of the overall treatment of the affected joint(s). The actual preparation for life with an artificial joint consisted of pre-operative rehabilitation care, where you learned, with the help of a physical therapist or doctor, the special exercises necessary to strengthen weakened muscles or muscle groups, or, conversely, to relax shortened and painful muscles. It was also important that you learned different types of walking with support on both high and French crutches and a cane. Do you feel that the pain in the operated joint has now completely subsided, and therefore neither exercise nor the use of a walking support is necessary? You are mistaken, overexertion of the operated joint would be comparable, with a little exaggeration, to trying to crack a nut in an artificial tooth from time to time. It could also become damaged or prematurely worn. The lifespan of a total hip replacement is also limited and a new surgery is required once it is damaged.
In order for your new hip joint to last as long as possible, it is necessary to follow certain rules even after you return from the hospital to your home or work environment. We will now introduce you to these rules.
In the early post-operative period, your doctor will usually recommend walking on high arm crutches with full relief of the operated lower limb. This means that the operated limb is virtually unburdened. This type of relief is achieved by so-called three-point walk. First, we move both crutches in front of you to about the distance of your short stride. When we are firmly supported on the crutches, the operated lower limb steps out (but must not step in front of the crutches), followed by the non-operated limb. Remember that when walking down the stairs, first move both crutches one step lower, then the operated lower limb steps out again, followed by the non-operated limb. Note that the opposite is true when walking up stairs! The non-operated lower limb steps first, we firmly stand on the crutches, bring the operated lower limb in and bring the crutches in last.
- Don't talk to anyone on the staircase!
- Don't look back, even if someone calls out to you.
- If you feel tired or unsure, insert rest breaks between walking.
- Don't hop down the stairs, don't jump!
Support
The height of any support, that is, French crutches and canes, must be appropriate to your body height. The high crutches must lightly touch your arm pits when standing, you must not lean towards them or hang on them. The appropriate length of French crutches is measured from the centre of your palm at the elbow of your slightly bent upper arm, with your forearm lightly touching the crutch socket. Walking sticks must also be neither too tall nor too short. With your elbow slightly bent (approximately 30 degrees), your palm should be touching the handle of the cane at your body. Remember that any new type of walking stick must be approved by your doctor!
- Don't be shy to practice walking in front of the mirror.
- Walk slowly, but in a natural rhythm.
- Beware of slippery and rough terrain.
- Take off your flip flops or even slippers, only sturdy shoes fastened over the heel will serve as suitable footwear.
- If your lower limbs are unequal in length, you should have the sole of the shoe increased to accommodate the shortened limb after consulting your doctor.
Mode of the day
Limit prolonged standing, especially in queues. Insert moments of sitting rest between walks. Remember that the hip joint is loaded approximately four times your body weight when walking. This load on the joint is compounded when standing. If your body weight exceeds the ideal figure (kilograms should correspond to approximately the number of centimetres of your height over 1 metre), try to reduce it reasonably.
- Do not copy different types of diets from friends.
- The appropriate diet will be recommended by your doctor.
- Adjust your work and home environment to reduce standing as much as possible. With the right height, or even angle, of the desk and the right type of higher or swivel chair (check it out at the dentist, for example), most work can be done just as well sitting as standing after some training. The same applies to housewives. In particular, learn to iron and prepare meals sitting down. A trolley bag is useful for essential shopping.
- In the postoperative period, do not sit for more than ½ hour, then change position.
- Don't sit with your leg over your foot. If you sit with the flat of your feet on the floor, place your feet far apart to prevent the knee and hip joints from rotating outwards.
- Adjust your bed so that it is higher and has a hard base, but is also soft and flexible with a mattress height of around 12 cm. A foam mattress is also suitable. Initially, sleep and turn over with a pillow between your thighs and knees.
Exercising
Regular daily exercise is an essential part of your treatment regime. Exercise lying down or sitting up on a suitable bed (hard but soft mat) in your workout clothes, preferably near an open window. Perform the exercises exactly as instructed. Learn each exercise in front of a mirror. Initially, repeat each exercise 3 times, gradually increasing to 10 times. The morning exercise is best suited to warm-up, while the second afternoon or evening exercise focuses more on the more difficult exercises. If you feel tired or more pain, shorten the exercise.
LYING ON YOUR BACK:
Contract the buttocks together for approximately 5 seconds, then relax the buttocks again for approximately 10-15 seconds.
From lying on the back with the lower limbs extended, pull the left lower limb towards the abdomen and replace it with the right one.
The knee joint of the bent lower limb must not be pulled towards the shoulder, rather towards the nose.
Never lift the lower limb extended!
Insert a small elastic cushion between the thighs and the knees, squeeze the cushion firmly with the thighs for about 5 seconds and release it again for about 10-15 seconds.
Alternate the left and right lower limbs. Neither the knee joint nor the leg itself must be externally rotated - the toe and the knee point upwards.
From lying on your back, gradually unwrap your head, neck and shoulder blades from the mat. Gradually put the shoulder blades, neck and head back on the mat. Individually, after some training, we can achieve a complete sitting position in this way. However, we never swing to sit.LYING ON THE BELLY
Contract the buttocks together for approximately 5 seconds, then relax the buttocks again for approximately 10-15 seconds.
Exten the left and right lower leg backwards alternately, the groin must remain pressed against the mat.
Alternately bend the left and right lower leg at the knee joint. The groin must again remain pressed against the mat, the bent limb must not point outwards or inwards.
Raise the torso up when inhaling and lower it again when exhaling.SITTING LEGS FREELY LOWERED
Stretch the upper limbs upwards and simultaneously lift the bent lower limb (alternating left and right).
Freely swing the left and right lower leg alternately with the buttocks pressed against the mat.
Inhale when turning the torso to the left, exhale when turning the torso to the right.
Insert breathing activities between each exercise. Combine active inhalation with movement of the upper limbs to the upright position, and during exhalation gradually increase the weight.Sports and recreational activities
In addition to regular exercise, swimming is particularly suitable as it strengthens muscles and increases the body's endurance and performance. Cycling on flat terrain is also possible. However, beware of falls. Be careful when getting in and out of the car. Only elevated seats are suitable for driving.
Finally, we wish you a lot of perseverance and success. Remember that everything goes better with a good mood.
- Conservative orthopaedic treatment
Joint arthrosis
What is osteoarthrosis?
Osteoarthrosis is a degenerative, non-inflammatory joint disease characterized by damage to the articular cartilage, sclerotization (thickening) of the bone under the cartilage, changes in the joint capsule and, as a result, deformation and limitation of joint mobility. Osteoarthritis is accompanied by pain, which depends on a number of factors, such as the degree of damage to the joint, the load, the presence of effusion in the hips, the weather, and the time of year.
Why does osteoarthrosis occur?
Arthrosis occurs in a joint where the balance between the cartilage's reparative abilities and the degree of load (damage) on the articular cartilage has been disturbed. In the so-called primary cause, the cause may not be clear. In secondary arthrosis, it results from damage to the menisci and ligaments, traumatic damage to the cartilage or axial changes in the limb after a bone fracture. It is also due to inflammatory diseases (rheumatoid arthritis, bacterial arthritis), neuromuscular or metabolic diseases.
Risk factors:
Age: arthrosis is the most common chronic disease of the elderly (80% of people over 75 are affected).
Sex: women are affected more often.
Weight or overweight: an increase in load while maintaining reparative capacity is associated with a higher incidence of arthrosis.
Conditions after injuries to joints or adjacent bones.
Additional factors: genetic disposition, geographical influences.
Which joint can arthrosis affect?
Basically every joint. Most often, however, the large joints of the lower limbs - the hip and knee joints, the intervertebral joints of the spine, the small joints of the hand, the root joints of the thumb and foot, less often the ankles, shoulders, elbows or wrists.
Can arthrosis be cured?
The treatment of arthrosis is quite difficult, in fact it cannot be cured completely. In severe forms, it can be helped by replacing the affected joint with an artificial one. In milder forms, the course of the disease can be influenced by changing the load and physical activities, reducing weight and increasing the resistance and regenerative capacity of the cartilage by appropriate pharmacotherapy.
The treatment of osteoarthritis is summarized in the recommendations of OARSI- the international professional society for osteoarthritis. Basically, it is a combination of regimen measures, pharmacological and surgical treatment. Regimen measures include, for example, adequate physical activity. Even the affected joint needs a certain amount of stress to provide nutrition to the articular cartilage. Conversely, excessive loading leads to cartilage damage. In obese people, weight reduction is important. Preventive treatment of joint damage or limb deformities (treatment of damaged menisci and ligaments, traumatic cartilage lesions, treatment of axial limb deformities). Use of appropriate orthopaedic equipment and other measures.
Which drugs can be taken for osteoarthritis?
Chondroprotection: called SYSADOAs, or disease-modifying drugs. These include, for example, glucosamine or chodroitin sulfate, MSM (methylsulfonylmethane), collagen, hyaluronic acid.
The advantage of these drugs is their minimal side effects and the study-proven effects on arthrosis.
By increasing the supply in the diet, cartilage regeneration can be improved. An anti-inflammatory effect and a reduction in pain have also been described. They are mostly freely available.Antireumatics: suitable in case of arthrosis decompensation (presence of swelling or effusion in the joint) or as an occasional analgesic. They may have side effects, most commonly on the gastrointestinal tract.
Pain-killers: they reduce pain in more severe forms of arthrosis, they do not affect the disease as such. These include, for example, Paralen, which according to the International Arthritis Society is the drug of first choice.
Injectables:
Application of growth factors, so-called autologous biological therapy: involves the activation of chondrocytes (cartilage cells) by growth factors. There is no clear evidence of its effectiveness or effect on the cause of the disease. However, it can be expected that in the near future this is where a major change in the treatment of this disease may occur. This treatment is not indicated for more severe forms of arthrosis and its disadvantage is the relatively high cost.
Hyaluronic acid application: intra-articular installation of this macromolecule improves the biochemical environment in the joint, which may lead to calming of arthrosis and stimulation of chondrocytes.
Corticosteroid application: when properly indicated, leads to calming of arthrosis, reduction of flow and prevention of effusion, which is subjectively perceived by a reduction in joint pain. If applied too frequently or incorrectly, it can, on the other hand, have a negative effect on the articular cartilage (injectable drugs must be administered by a doctor, preferably an orthopaedic surgeon).
Surgical treatment:
THR - total joint replacement: nowadays it is one of the most common and basic operations performed in orthopaedic departments. With the improvement of THP implants, surgical procedures and techniques, and last but not least, the intensification of rehabilitation, this type of surgery is displacing other surgeries (osteotomies and arthrodesis) and is performed even in younger patients. Further information can be found in the " patient information" folder.
UNI THR - unicompartmental joint replacement: ½ knee replacement: is indicated in case of damage to the inside or outside of the knee. This operation has a number of advantages (minimally invasive surgical approach, easier rehabilitation), but has relatively narrow indication criteria.
Other surgical procedures for osteoarthritis: ASK, osteotomies, arthrodesis.
Treatment of osteoarthrosis of the joints according to OARSI recommendations/International Osteoarthritis Society.
Nonpharmacological:
Combination of nonpharmacological treatment and pharmacotherapy
- Patient education, lifestyle modification.
- Regular telephone checks.
- Examination by a physiotherapist and exercise instruction.
- Regular exercise
- Weight reduction in obese people.
- Support aids (canes, crutches).
- Orthoses for joint instabilities.
- Medical shoes and orthopaedic insoles.
- Application of heat.
- TENS-transcutaneous electrical nerve stimulation.
- Acupuncture.
Pharmacotherapy:
- Paracetamol-paralen in doses up to 3g per day.
- Non-steroidal antirheumatic drugs - NSAIDs.
- Topical NSAIDs and capsaicin in knee arthrosis.
- Intra-articular injection of glucocorticoids.
- Intra-articular injection of hyaluronic acid.
- Glucosamine and chondroitin sulfate for pain relief.
- Glucosamine, chondroitin and diacerein-probable structural effect.
- Weak and moderate opioids.
Surgical treatment:
- Total joint replacement.
- Unicompartmental joint replacements.
- Osteotomy and preventive joint surgery.
- Joint lavage and arthroscopic treatment in gonarthrosis.
- Arthrodesis.
- Patient education meeting before THR
Dear patients,
If you are facing a knee or hip THR, you can come to the meetings we regularly hold for patients. At these meetings, you will learn more about the procedure you are about to have, what to arrange before you are admitted to hospital, and what you need to provide for after the operation. We will go through everything with you step by step, the different stages of the hospitalisation from the day of admission until discharge. This includes instruction and demonstration of the use of French canes and other aids by our physiotherapist. Of course, we will answer your questions, give you advice and help you.Check the news on the main page for meeting dates.
- Minimally Invasive Foot Surgery - MICA
Since 2022, our workplace has been performing new minimally invasive forefoot surgeries - most commonly correction of bunions and flat feet, correction of deformities of other toes, or treatment of degenerative diseases of small joints of the foot. The new method involves the use of special cutters and modern implants. The minimally invasive surgery offers a lower risk of complications, faster healing and therefore an earlier return to a normal way of life compared to conventional "open" procedures.
Orthopaedic Department